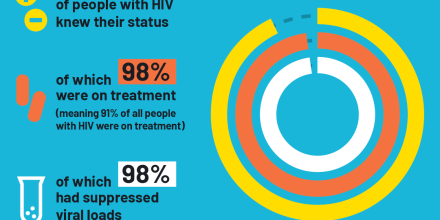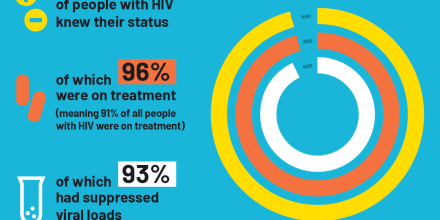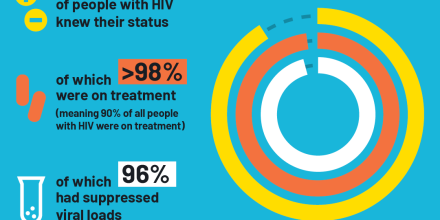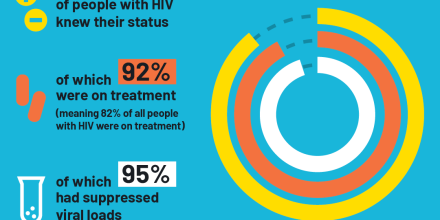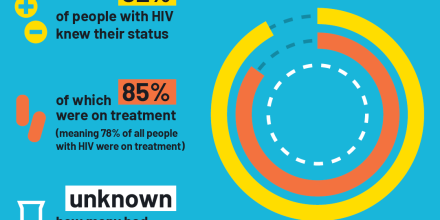
At a glance: HIV in Kenya
Understanding the HIV epidemic
Hester Phillips
11 April 2023
Interviews with young LGBTQI+ people in Bangladesh describe experiences of stigma in everyday life – and the power of positive representation and friendship
New research highlights how young LGBTQI+ people in Bangladesh have little support at home, in public or within healthcare. But friendships with other LGBTQI + people and positive media representation helps them cope.
How young LGBTQI+ people in Bangladesh deal with social expectations and pressures to be heterosexual and conform to gender norms. (Gender norms are about saying how men and woman should look and behave.)
Researchers interviewed 14 young people (ages 18 to 24) from Dhaka who identify as lesbian, gay, bisexual, transgender or queer.
Young LGBTQI+ people face stigma and discrimination. This affects their quality of life. It also increases their risk of health issues, including HIV, sexually transmitted infections and mental health conditions. Despite this, young LGBTQI+ people are often ignored in health research. Particularly in places where they are criminalised, like Bangladesh.
Interviewees felt pressure from families to get married to someone of the opposite sex. They said young women in Bangladesh particularly face this pressure.
This has harmful consequences. Armina, a 21-year-old lesbian woman, described feeling “mental torture” due to family pressure to marry a man. This made her consider suicide.
Badol, a 20-year-old transgender man, was forced by his family to marry a man. The marriage was abusive. Badol left, only to experience further violence from his father in an attempt to ‘straighten’ him up.
Some interviewees experienced verbal and physical harassment in public.
Interviewees who were publicly harassed said it was because they were seen as feminine. For example, Shayan, a 24-year-old who gay man, was publicly harassed for having long hair. But interviewees said that women presenting as masculine were likely to get a positive reaction as they were considered to be “upgrading” from female to male.
These experiences affected young people’s wellbeing. Some limited where they went and with whom. They avoided public transport and going out alone and chose to socialise at friends’ homes. Some felt unable to be themselves in public, which led to guilt and shame.
Interviewees experienced harassment in health facilities. This was particularly the case for transgender interviewees. They were disrespected and stigmatised for their gender identity, even when this is what they were trying to get medical support for.
Two transgender interviewees had psychiatrists treat their gender identity as a mental illness. Trishna, a 24-year-old transgender woman, was given medication that left her unable to enjoy life or to work.
Most interviewees preferred to use an LGBTQI + friendly doctor for sexual health issues. But some said that the murder of Xulhaz Mannan in 2016, who had set up a sexual health referral service for LGBTQI+ people, had made it harder to access these services.
Interviewees reported feeling internalised homophobia when growing up. For example, feeling “unnatural”, “dirty”, “gross” and “not normal”. Many felt confused about their sexuality and gender identity from a young age. They described being seen as different by their peers, which led to bullying. Transgender interviewees described feeling physically uncomfortable in their bodies during their childhood and teenage years.
These experiences affected interviewees’ mental health. One said it caused them to attempt suicide.
Interviewees coped by finding support from peers, television shows and the internet. They said that seeing other LGBTQI+ people helped them to feel more comfortable with who they were. Some gave examples of specific Hindi and English television shows that helped them. Forming online and in-person friendships with other LGBTQI+ people was seen as very important, especially when first learning about sexual and gender diversity.
Trishna said: “I made a lot of friends online. …It helped me to stop my suicidal addiction. …When I saw that I wasn’t alone. There are many people who are facing similar situations. This is normal. I felt relieved after that.”
The study shows the power of friendship for young LGBTQI+ people. Working with peer educators can be an effective way to get HIV and sexual health services to young LGBTQI+ people. Especially if they are stigmatised and struggling to access appropriate care in health facilities.
It also shows the power of positive media representation. It can be effective to use ‘edutainment’ products, such as online films, television and radio content, which accurately represent young LGBTQI+ people. This can be a powerful way to communicate sexual health messages and help young LGBTQI+ people feel comfortable with who they are.
Tailored mental health screening and support should also be provided as part of sexual health and HIV services if possible. Or referrals made to mental health services which are sensitive to the needs and feelings of LGBTQI+ people.
It is also essential to challenge the laws and social norms that criminalise and stigmatise LGBTQI+ people, which has clear consequences for their health and wellbeing.
Keep up-to-date with all our latest news stories and blogs by signing up to the Be in the KNOW news digest.